|
About this page
Archive news page, covering events, conferences and non-product specific news items from 2002. |
Contents
|
|
Last updated: May 2003 Revision: 1.2 |
An international advisory group of scar management experts have recently published evidence-based recommendations that support the use of silicone gel sheeting as a first-line therapy on immature, linear and widespread burn hypertrophic scars, and minor keloids [1]. Silicone gel sheeting should also be considered as a first-line prophylactic measure to help prevent the development of hypertrophic or keloid scars after surgery.
Over 300 published references on scar management were reviewed. Analysis based on the results from at least eight randomised controlled trials and a meta-study of 27 trials confirmed that silicone gel sheeting is a safe and effective management option for hypertrophic scars and keloids.
Early diagnosis can reduce the risk of a problem scar evolving. The authors conclude that the most successful treatment of a hypertrophic scar or keloid is achieved when the scar is immature but with the overlying epithelium intact, although this is not as yet confirmed in the current literature. Prophylactic use of silicone gel sheeting should begin soon after surgical closure, when the incision has fully epithelialised, and be continued for at least one month.
Mustoe TA, Cooter RD, Gold MH, Hobbs FDR, et al. International Clinical Recommendations on Scar Management. Plastic and Reconstructive Surgery 2002;110:560-71. Available from http://www.plasreconsurg.com/article.asp?ISSN=0032-1052&VOL=110&ISS=2&PAGE=560
This seminar will review the development of a sound scientific foundation for understanding the aetiology of pressure ulcers, and outline promising approaches for their prevention.
The day will be broken down in to four sessions:
Cell and tissue biomechanics
Technical equipment
Pathophysiology
Imaging and monitoring
It is aimed at engineers and clinicians and will highlight opportunities for applying new technologies to study the problem in terms of the interaction between biomechanical and physiological factors.
For further information and to download the Programme and Registration Form please visit:
http://www.imeche.org.uk/conferencesandevents/
Alternatively contact:
Madeline Willis, Events Assistant, IMechE, 1 Birdcage Walk, London SW1H 9JJ Tel: +44 (0)20 7973 1260 Fax: +44 (0)20 7233 1654 Email: m_willis@imeche.org.uk
A study published in the Lancet [1] has shown that hormone replacement therapy may help prevent leg ulcers in women over the age of 65 years.
This study involved 44,195 elderly women, aged between 65 and 95 years, taken from the UK General Practice Research Database. Venous leg ulcers occurred in 1744 women and pressure ulcers in 802 women. Of the 4944 women receiving HRT, 108 developed a venous leg ulcer, and 49 developed a pressure ulcer. Women who received HRT were found to be significantly (30-40%) less likely to develop a venous leg ulcer or a pressure ulcer than non-users.
This observational study would appear to provide early evidence that HRT could have a beneficial effect in preventing chronic wounds.
Margolis DJ, Knauss J, Bilker W. Hormone replacement therapy and revention of pressure ulcers and venous ulcers. Lancet 2002;359:675-677.
Wound bed preparation (WBP) is defined as the 'removal of local barriers to healing'.
WBP provides a clinical framework for rationalising wound care and ensuring that optimal success is achieved with current therapeutic modalities. Opinion leaders worldwide are committed to the concept of WBP.
Smith & Nephew has launched an interactive, educational website www.GlobalWoundAcademy.com, designed to develop and disseminate the concept of WBP. In addition, they hosted a series of four ground breaking symposia at venues across the UK with keynote presentations from Dr Vincent Falanga and Dr Gary Sibbald. Further presentations on aspects of WBP were given by other eminent experts in wound care including Professor Keith Harding, Caroline Dowsett, and Kathryn Vowden. Over 1000 members of the nursing and medical community attended, providing a major platform for discussion and debate.
Dr Falanga states that: "Wound bed preparation is emerging as an essential element for obtaining maximal benefits from today's advanced wound care products'. This view is supported by Dr Sibbald who says: "Debridement, bacterial balance and moist interactive healing must all be optimised as integral parts of preparing the wound bed."
Within Smith & Nephew the WBP category comprises a range of products and extended product offerings. These are available for the professional user, providing cost-effective topical site management of all wounds that contain a barrier to healing.
In an article on World Wide Wounds, made possible by an educational grant from Smith & Nephew, Kathryn and Peter Vowden discuss the five key components of WBP. These are:
Removal of necrotic burden
Removal of bacterial burden
Optimising exudate levels
Removal of the cellular burden
Correction of biochemical imbalances.
WBP is a dynamic process and the status of the wound bed needs to be assessed continuously until complete healing is achieved. Restoration of bacterial balance is one of the key aspects of effective WBP.
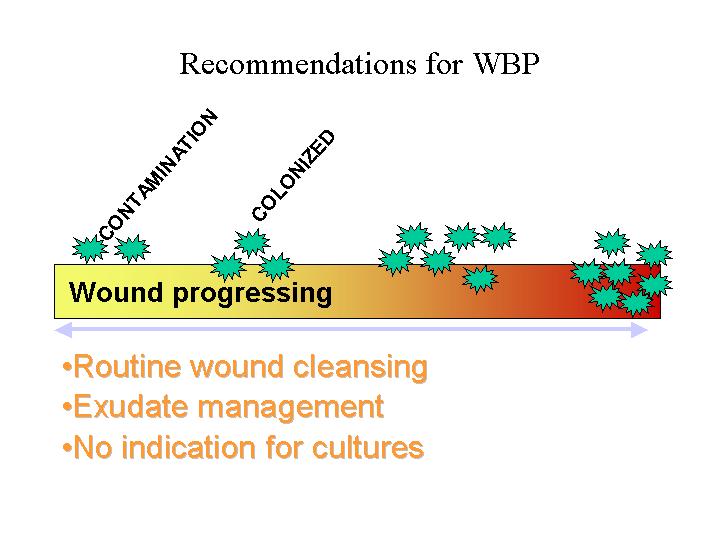
All chronic wounds contain bacteria. The presence of bacteria in the wound does not, however, indicate infection or a barrier to wound healing. The impact of bacteria on healing will depend on the pathogenicity of the organism, the bacterial load, the toxin produced and the host response. It is helpful to assess the impact of bacteria using the continuum given in the figure below. This shows the impact of severity, ranging from contamination to infection.
The challenge to the clinician lies in identifying the state of the wound in relation to this continuum.
Contamination is the presence of non-replicating bacteria within the wound and is a normal condition in chronic wounds. The fact that wounds are contaminated does not contribute to impaired healing.
Colonisation is the presence of replicating bacteria without host reaction.
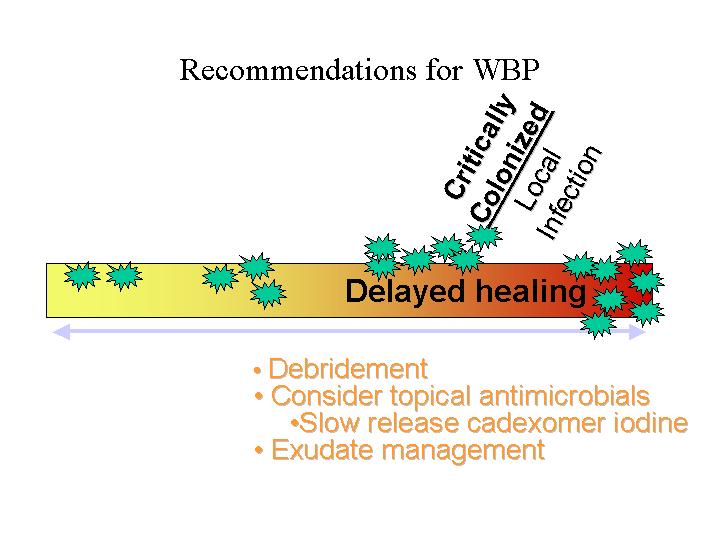
Critical colonisation is where there are no systemic signs of infection, but rather subtle local signs. This may be a change in the equilibrium or an increasing bioburden contributing to delayed healing.
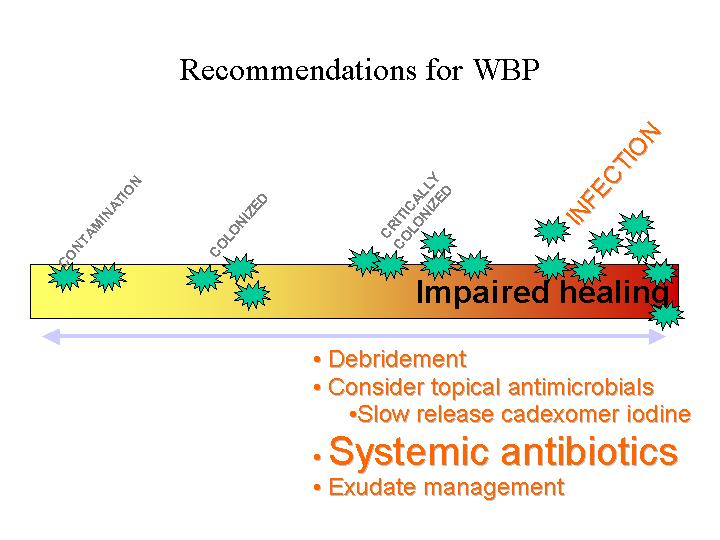
Clinical infection is considered present when the bacteria have invaded the tissue, are multiplying and causing a systemic host reaction and impaired healing.
It is only as the bacterial load moves to the right of this continuum that bacteria start to impair wound healing. Recommendations for WBP are illustrated in the figures below (click on the images to see them at full size):
Bacteria can affect healing at several stages of the healing process, causing the following:
Disordered leukocyte function
Disruption in normal clotting mechanisms
Prolonged inflammatory phase
Less efficient angiogenesis
Altered granulation tissue formation.
WBP is an all encompassing concept, ensuring that wound management focuses on both the wound itself and the patient as a whole. This involves using a holistic approach to care. It is important for the clinician to address both the host systemic complications and the underlying wound healing complications such as deep-rooted infection.
When bacteria proliferate, increasing the bacterial load to greater than 105, wound healing is impaired. It is recommended that systemic antibiotics are used together with sustained release topical antimicrobials (for example silver sulphadiazine or cadexomer iodine) [1]. Therapy should be based on the clinical status of the patient and the wound, as opposed to the microbiological assessment alone.
Cadexomer iodine:
Iodine plays a natural role in the body's immune system and in fighting infection. It serves as a halide, which is needed for neutrophils to exert their action during the inflammatory phase of healing. Cadexomer iodine (cadexomer beads with 0.9% iodine, Iodoflex) is a topical preparation which helps to address all the main barriers to healing. It has a unique mode of action, described by Falanga as a SMART release system [2], whereby the cadexomer beads actively respond to exudate by releasing iodine in a controlled sustained manner, providing broad spectrum antimicrobial activity for up to three days [3]. The iodine is deactivated by organic matter in the wound, detected by the cadexomer carrier, which in turn releases more iodine. This ensures that there is always a greater concentration of iodine in the dressing than at the wound site, thereby avoiding any cellular toxicity, which has been a problem with traditional antimicrobial preparations.
It has been demonstrated, beyond reasonable doubt, that CI is non-toxic to cells both in vitro and in vivo. In a study by Zhou et al, histological assessment of chronic wound cells following CI treatment revealed no cell necrosis or morphological changes [4]. Falanga states that the propaganda of the 1980s about the toxicity of antiseptics was based on the inappropriate use of traditional antiseptic agents (e.g. povidone iodine), which release their complete load of iodine in one short action resulting in cellular toxicity [2].
Other advantages of using CI include:
assists in debridement and absorption of high levels of exudate (up to 6 ml/g of dressing), making it a highly versatile agent and an integral part of WBP
reduces problems with dressing removal - cadexomer beads are naturally derived from starch molecules which allow any remnants of the dressing to biodegrade.
Falanga states that 'Judicious use of iodine antiseptics promotes wound bed preparation and accelerates wound healing ... CI is an effective debridement and antiseptic agent for chronic exudative wounds. When used directly over the wound CI removes pus, debris and wound exudate and effectively reduces the bacterial counts' [2].
Finally, Carita Hansson has shown that if the instructions for correct use are followed, CI is an effective therapy which decreases the microbial burden, cleans the ulcer from slough and exudate and promotes healing [5].
Silver sulphadiazine:
Silver sulphadiazine (Flamazine) is another useful antimicrobial agent. By releasing silver into the wound bed, SSD helps to address the bacterial burden and prepares the wound bed for fast, cost-effective healing of chronic wounds [6], [7].
SSD forms the mainstay of topical burns therapy and its use is often overlooked in chronic wound treatment. It has, however, proved to be beneficial in the treatment of chronic wounds [2], in both treating and preventing infection [8]. Unlike other silver containing products on the market, SSD releases silver slowly from the oil in water formulation in concentrations that are selectively toxic to micro-organisms and is useful for use on low exuding wounds.
Kucan et al have compared the topical use of saline, povidone iodine and SSD on pressure ulcers [9]. SSD was found to be 100% successful in reducing bacterial contamination down to less than 105 compared to 79% for saline, and only 64% with povidone iodine.
SSD is a broad spectrum antimicrobial and many authors are now advocating its use against MRSA [10]. Salman and Leakey [11] have shown that out of 103 MRSA clinical isolates tested there were no reports of MRSA showing resistance to SSD.
In the UK, nurses who have undergone the advanced nurse prescribing course can now prescribe SSD.
Over time, the status of the wound will vary. WBP is therefore a dynamic, continuous process that runs in parallel with wound healing. The different elements of WBP should not be treated in isolation. In achieving good WBP, it is important to accurately assess and monitor the impact of bacteria on the wound and to institute local or systemic therapy as indicated.
Smith & Nephew offer solutions for all healthcare professionals woundcare needs. To find out more please contact the helpline on 0800 590173.
Clinicians should consider the use of the two highly effective antimicrobial agents described in this advertorial, both of which are supported by substantial clinical evidence and experience. For best results, SSD should be used in non- to low exuding wounds, whilst CI should be used in moderate to highly exuding wounds. Both form integral parts of WBP through removal of local barriers to healing.
The views expressed in this advertorial are those of Smith & Nephew and are not necessarily those of the publishers.
Sibbald RG, Williamson D, Orsted HL, et al. Preparing the wound bed - debridement, bacterial balance and moisture balance. Ostomy Wound Manage 2000; 46: 14-35.
Mertz PM et al. The wound environment: implications from research studies for healing and infection. Wounds 1996; 8 (1): 1-8.
Zhou LH, Nahm WK, Badiavas E, et al. Slow release iodine preparation and wound healing: in vitro effects consistent with lack of in vivo toxicity in human chronic wounds. Br J Dermatol 2002; 146: 365-367.
Hansson C. The effects of cadexomer iodine paste in the treatment of venous leg ulcers compared with hydrocolloid dressing and paraffin gauze dressing. Int J Dermatol 1998; 37: 390-96.
Kjolseth D, Frank JM, Barker JH et al. Comparison of the effects of commonly used wound agents on epithelialization and neovascularization. J Am Coll Surg 1994; 179 (3): 305-12.
Geronemus RG, Mertz PM, Eaglstein WH et al. Wound healing. The effects of topical antimicrobial agents. Arch Dermatol 1979; 115; 1311-14.
Bishop JB, Phillips LG, Mustoe TA et al. A prospective randomised evaluator-blinded trial of two potential wound healing agents for the treatment of venous stasis ulcers. J Vasc Surgery 1992; 16; 251-57.
Kucan JO et al. Comparison of silver sulphadiazine, povidone iodine and physiologic saline in the treatment of chronic pressure ulcers. J Am Geriatr Soc 1981; 29: 232.
Young T. Managing MRSA wound infection and colonisation. Nurs Times 2000; 96 (4); 14-16.
Preventing trauma to the wound and pain to the patient were considered to be the main concerns in a multinational wound care survey recently conducted.
Nearly 4,000 practitioners from eleven countries across Europe and North America took part in the survey, the results of which were announced at the 12th annual congress of the European Wound Management Association (EWMA) 23-25 May 2002 in Granada, Spain.
Practitioners consistently ranked dressing removal as the time of greatest pain. And pain free removal was the most highly desired characteristic of a dressing, with five countries considering it the most important factor.
Seven of the countries ranked preventing trauma as the most important consideration in their approach to pain.
Christine Moffatt, president of EWMA, says the findings raise important issues for wound care professionals and advocates the use of dressings such as soft silicone products which promote pain free removal.
"Research in the last ten years has focused on healing as the major outcome of treatment, the next decade must focus on the patient with pain management a priority," says Christine Moffatt, professor of nursing at Thames Valley University, London, and Co-director of the Centre for Research and Implementation of Clinical Practice.
To help redress this problem EWMA has produced a position document on pain at wound dressing changes.
The position document is peer reviewed and contains full details of the multinational survey, an explanation of the complex underlying mechanisms involved in acute and chronic pain, and a guide to the management of procedural pain. It is available in English, French, German, Italian and Spanish.
"We hope that this document will stimulate international discussion and lead to collaboration and tangible benefits to patients, clinicians and the industry," says Professor Moffatt.
Both the survey and the position document have been supported by an educational grant from Mölnlycke Health Care.
`Pain at Wound Dressing Changes' is EWMA's first position document, made possible by an educational grant from Mölnlycke Health Care. The aim of a position document is to:
provide clear clinical advice and recommendations for practice
produce a literature review presented by international experts
highlight future questions for research and practice
have wide dissemination and availability in different languages (English, French, German, Italian and Spanish).
`Pain at Wound Dressing Changes' provides a comprehensive review on this important topic. The papers collectively form a free educational resource, which can be used to update clinicians in many different countries.
Each of the translated versions has a foreword written by a key opinion leader from the country concerned. They are: France - Sylvie Meaume (Specialist in Dermatology and Gerontology); Italy - Marco Romanelli (Consultant Dermatologist); Spain - Javier Solevilla Agreda (Professor of Geriatric Care) and Joan-Enric Torra i Bou (Coordinator, Interdisciplinary Chronic Wounds Unit); Germany - Wolfgang Vanscheidt (Professor of Dermatology).
The content includes three key articles which will be described below:
Written by CJ Moffatt, PJ Franks, H Hollinworth
This article discusses the results of an international collaborative survey which sought to explore practitioners' understanding of pain and trauma at wound dressing changes.
Key findings
Dressing removal is considered to be the time of most pain.
Dried out dressings and adherent products are most likely to cause pain and trauma at dressing changes.
Products designed to be non-traumatic are most frequently used to prevent tissue trauma.
Gauze is most likely to cause pain. New products such as hydrogels, hydrofibres, alginates and soft silicone dressings are least likely to cause pain.
Awareness of product range and ability to select dressings is highly variable between countries.
Use of valid pain assessment tools is considered a low priority in assessment with greater reliance on body language and non-verbal cues.
Written by H Wulf, R Baron
This article explores the complex nature of the underlying mechanisms involved in both nociceptive (inflammatory) and neuropathic pain to enhance our understanding of patients' pain experiences.
Key points
The pathophysiology of pain involves an alteration of pain transmission pathways.
Tissue damage and inflammation sensitises nerve endings that transmit pain signals.
Increased sensitivity of neurons to a repeated stimulus can cause benign sensations to become painful.
Injury to the peripheral nerves is often associated with abnormal sensory function, causing a marked increase in patients' perception of pain.
An understanding of how the nervous system responds and adapts to pain is vital if we are to make sense of patients' pain experiences.
Written by M Briggs, JE Torra i Bou
This paper draws on the authors' clinical experience and the basic science of pain physiology to offer recommendations for good practice when managing pain at wound dressing changes. Because of the complexity and size of the topic, the focus is specifically on managing pain at dressing removal in adult patients with chronic and non-burn wounds.
Key points
Pain control methods at wound dressing changes are often under-utilised by practitioners.
Pain arising from wounds is multidimensional in nature and practitioners should adopt a broad holistic approach to management.
It is vital that patients are supported by a combination of techniques to help them through the dressing procedure including good preparation, appropriate choice of dressing materials and adequate analgesia.
In addition the following strategies are suggested for the relief of pain at dressing changes:
| Avoid any unnecessary stimulus to the wound, such as drafts from open windows, prodding, poking |
| Handle wounds gently, being aware that any slight touch can cause pain |
Select a dressing
which:
|
Reconsider dressing choice
if:
|
Read manufacturers' instructions about technique for removal |
In the multinational survey the most important strategy to avoid wound damage was the use of non-traumatic dressings and was the only question on which there was complete agreement. However, the survey also highlighted the variation in knowledge, with many practitioners unaware of the products specifically designed for prevention of wound pain and trauma.
Reducing the pain during dressing changes is a major priority when it comes to patient's quality of life, optimising wound healing, and the overall cost of treatment.
Mölnlycke Health Care have developed the Tendra® range of soft silicone wound dressings with Safetac® technology. These include: Mepitel®, Mepilex®, Mepilex® Border and Mepilex® Transfer.
Features include ability to:
minimise trauma to the wound and pain to the patient at dressing removal [1], [2], [3]
maintain a moist wound environment
be cost effective [3].
Mepitel - a soft silicone wound contact layer with an open mesh structure which allows excess exudate to pass into an outer absorbent dressing.
It can be used on a wide range of wounds including:
traumatic wounds such as skin tears, abrasions and second degree burns
chronic wounds
fixation of grafts.
Mepilex - a soft silicone foam dressing with a moisture/vapour-permeable waterproof film backing. It effectively absorbs large amounts of exudate.
It is indicated for use with:
a wide range of exuding wounds such as leg and foot ulcers
traumatic wounds such as skin tears, abrasions and burns.
It is suitable for use under compression bandaging.
Mepilex Border - a self-adherent soft silicone foam dressing.
It is indicated for use with:
a wide range of exuding wounds such as pressure ulcers, leg and foot ulcers
traumatic wounds.
Mepilex Transfer - a soft silicone exudate transfer dressing. It consists of a flexible and hydrophilic polyurethane foam coated with a soft silicone layer.
It is designed for use with:
a wide range of exuding and difficult-to-dress wounds such as fungating wounds and epidermolysis bullosa.
'Pain at wound dressing changes' is available from www.tendra.com (pdf format). The document is available in English, French, German, Italian and Spanish.
![]()
The views expressed in this advertorial are those of Mölnlycke Health Care and are not necessarily those of the publishers.
Dahlstrom KK. A new silicone rubber dressing used as a temporary dressing before delayed split skin grafting. Scand J Plast Reconstr Hand Surg 1995; 29: 325-27.
Platt AJ, Phipps A, Judkins K. A comparative study of silicone net dressing and paraffin gauze dressing in skin-grafted sites. Burns 1996; 22(7): 543-45.
Gotschall S, Morrisson MIS, Eichelberger MR. Prospective, randomised study of the efficacy of Mepitel? on children with partial thickness scalds. J Burn Care Rehab 1998; 19(4): 543-45.
Dykes PJ, Heggie R, Hill SA. Effects of adhesive dressings on the stratum corneum of the skin. J Wound Care 2001; 10(1): 7-10.
World Wide Wounds invites you to send press releases about new developments related to wound management.
Please send your text by email to
www.editor@smtl.co.uk