
|
Author(s)
Jackie Stephen-Haynes
|
Contents
|
|
Published:
October 2007
Last updated: October 2007 Revision: 1.0 |
Keywords: leg ulcers; chronic wounds; frameworks; acronyms; wound bed preparation; TIME; holistic assessment.
The concept of wound bed preparation and the TIME framework (Tissue management; Inflammation and infection control; Moisture balance; Epithelial (edge) advancement) offer a logical and systematic approach to the assessment and delivery of wound care for patients with leg ulceration.
Wound bed preparation and the TIME framework must be used as part of an integrated approach, including differential diagnosis, prevention of recurrence and management of psychosocial issues.
Future work needs to focus on evaluating the effectiveness of such frameworks and refining them to best suit the clinical environment.
Significant advances have been made over the past two decades in the delivery of effective services for patients with leg ulceration. Treatment costs, however, remain high and the development of strategies to ensure future provision of effective care is important. Recent research into conditions at the wound bed has focused attention on the benefits of wound bed preparation and the use of the TIME framework to underpin care. Developed as a result of consensus meetings with key wound care opinion leaders, TIME offers a logical and systematic approach to the assessment and management of the wound bed, guiding practitioners in linking clinical observations and clinical outcomes. However, it is of limited value if clinicians fail to use it as part of an holistic approach. This paper explores additional factors that need to be considered alongside wound bed preparation and the TIME framework in order for care to be effective.
The past 20 years have seen a significant shift towards the delivery of evidence-based leg ulcer care and improved healing rates for many patients. Recent interest in chronic wound healing has led to a clearer understanding of cellular and molecular imbalances present in the wound bed that may contribute to delayed healing for some patients [1] [2]. Wound bed preparation - a concept aimed at assisting clinicians in wound bed assessment and the development of strategies to maximise healing potential - is now recognised as an important aspect of care. The associated development of the TIME framework (Tissue management; Inflammation and infection control; Moisture balance; Epithelial (edge) advancement) [3] offers clinicians a practical tool for translating wound bed preparation into practice.
The success of wound bed preparation and the TIME framework in improving patient outcomes is dependent on their value in clinical practice. An holistic approach is central to effective care [3]. Other factors to consider alongside the wound bed include the skin, the limb, vascular supply, pain and ulcer aetiology [4], as well as the patient's health beliefs, level of understanding and concordance.
Leg ulceration is a common, difficult and expensive health problem, affecting 1-2% of the population [5] [6] [7], and representing a significant challenge to the health service. A third of patients develop their ulcer before the age of 50 [5] and 2% of those over 80 years of age are thought to suffer with this condition [8]. Recurrence rates are high: 26% after one year and 31% after 18 months of healing for venous ulcer patients [9]. The cost burden to the NHS has been estimated at around £400 million per annum [10] and numerous studies have identified the negative impact on patient quality of life [11] [12] [13]. Prevalence of leg ulceration and the associated demands on service provision are likely to remain a challenge, due not only to these high recurrence rates but also as a consequence of an ageing population and the rise in chronic conditions such as obesity and diabetes.
Over recent decades service provision has become more rationalised and models of care have been developed. In the UK, most patients with leg ulceration are treated by nurses in the primary care setting, usually in their own homes [5]. It is important that primary care trusts (PCTs) are responsible for modelling services around the needs and profile of their patient groups. Moffatt et al [14] identified the benefits of leg ulcer clinics, where patients receive appropriate assessment and management and where a robust referral system to a member of the multi-professional team is in place. Clinics afford the adoption of leg ulcer guidelines and the opportunity to develop 'one-stop' assessment centres that incorporate investigations such as Duplex scanning and access to vascular surgeons [15]. The Lindsay Leg Club Model [12] recognises the importance of holistic care for patients with or at risk of leg ulceration and is based on a social model of 'leg health'. Services are delivered in a non-medical setting with an emphasis on 'drop-in', social interaction, participation, empathy and peer support.
The quest for effective frameworks of care continues. Service delivery and choice of setting varies across the UK and even within individual PCTs. Factors that may influence future developments include the increase in the number of older people as the population ages, as well as growing financial constraints within the health service. It is important that directors within health service organisations engage with the needs of patients with leg ulceration, and that clinicians are well educated, utilise local and national guidelines and continue to network in order to strive for delivery of a high-quality, systematic and effective approach to care.
Wound bed preparation is a rapidly emerging concept [16] that has recently gained popularity among practitioners. It represents a model of care for the management of chronic wounds based on the observation that cellular and molecular imbalances at the wound bed may contribute to delayed healing [3]. The TIME acronym - inspired by Falanga's original work and further developed by EWMA (European Wound Management Association) following consensus meetings with key opinion leaders [3] - comprises the four components of wound bed preparation and offers a logical and systematic framework (Box 1). It guides clinicians to consider each of these key clinical areas in monitoring the wound, decision making and the use of targeted interventions.
It has always been stressed that the original concept of wound bed preparation must be part of an ongoing, holistic wound management strategy [3]. It could, however, be argued that in some areas of practice clinicians focus mainly on the wound and less attention is paid to assessment, underlying aetiology and the management of psychosocial issues.
The success of any framework is largely dependent on the way individual practitioners interpret and integrate it in practice. While frameworks cannot replace good clinical judgement or make up for poor clinical skills, they offer an aide-mémoire [17] [18]. They also present clinicians with a useful means of providing evidence of care and of ensuring assessments are standardised between practitioners. Future research needs to focus on evaluating the uptake of wound bed preparation and the TIME framework in clinical practice and its effect on patient care. Evaluation of similar frameworks such as pressure ulcer risk assessment tools suggest that they are widely used and valued in clinical practice and that their limitations are not necessarily problematic in the clinical environment [18].
A possible limitation of the TIME framework is that it might encourage an emphasis on the wound bed to the detriment of wider issues such as ulcer aetiology and the patient's psychosocial well-being. While attempts have been made to include the TIME framework within the context of total patient care (Figure 1)(Figure 2), there are some key elements of assessment and management that may not receive an equal focus.
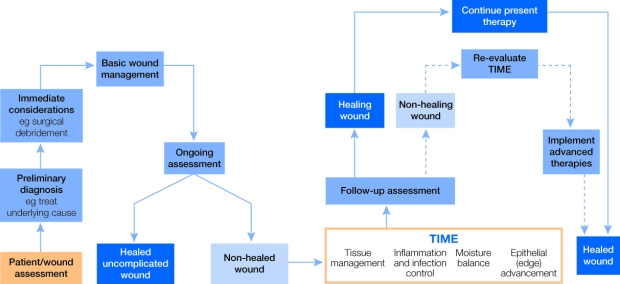
Leg ulceration is recognised as a multi-faceted problem requiring a holistic approach (Box 2). Early diagnosis and implementation of therapies required for healing and wound bed preparation are essential.
Reproduced from Morison et al (1999) [18].
The development of an additional framework that addresses other key elements of care, used alongside the original TIME framework, may help encourage a more holistic approach to leg ulcer management. This might include:
The concept of quality of life reflects an individual's level of satisfaction with various aspects of daily life, including housing, environment, recreation, health and well-being [19]. Leg ulceration can impact significantly on a person's quality of life, affecting physical and social functioning as well as psychological well-being [19]. Patients report increased pain, restrictions around what they can wear, limitations to their social lives, low self-esteem, depression and social stigma [12].
An understanding of the impact of the ulcer on quality of life and the development of realistic patient-focused outcomes is important if concordance is to be achieved [12] [13]. Poor regard for patient concerns may be particularly difficult where healing is not a realistic outcome and the focus is on chronic disease management. Negotiation may be required to find a treatment that is both comfortable and effective [20].
Patient education and active participation in treatment are important aspects of care and may improve concordance [21] [22].
Pain and discomfort are frequently associated with leg ulceration regardless of aetiology and may be linked to poor concordance [20] [23] [24] [25]. Ongoing, systematic pain assessment and management, as well as timely referral for specialist input where required [26] [27], are integral to holistic care and should be adequately documented [28]. An individual's experience of pain is unique, complex and influenced by many factors, although ability to effectively communicate these details may vary considerably between patients. Practitioners should assume that all wounds are painful or can become painful over time, that the surrounding skin may be sensitive, and that even the lightest touch may be intensely painful [26] [27]. The World Union of Wound Healing Societies (WUWHS) and EWMA consensus documents on wound-related pain provide invaluable guidance to clinicians [26] [27]. Hollinworth [29] offers a practical template for assessment of procedural pain, as well as strategies to minimise pain at dressing changes, including:
Successful leg ulcer management is dependent on accurate diagnosis of the underlying pathophysiology (ulcer aetiology) and subsequent targeted interventions. Venous hypertension and arterial insufficiency are widely accepted as the most common causes [30], with many patients experiencing mixed venous/arterial ulceration [1] [31]. Less common causes include, among others, rheumatoid arthritis (9%), diabetes (2.5%) [32], pyoderma gangrenosum, necrobiosis lipoidica, vasculitis, erythema induratum, cellulitis, bullous pemphigoid and skin cancer [33].
Clinical intervention at the wound bed without adequate measures to understand and manage the ulcer aetiology represents an ineffective and potentially detrimental approach to care. Clinicians should be aware of skin and lower limb changes that may indicate the underlying aetiology, as well as associated risk factors. Where diagnosis is difficult, prompt referral to a specialist is required. An holistic framework is important in establishing ulcer aetiology and national Royal College of Nursing (RCN) and Scottish Intercollegiate Guidelines Network (SIGN) guidelines offer documentation that can be used to inform diagnosis [31] [34]. Clinicians should be familiar with local, national and international guidelines and referral pathways.
Effective care should be targeted at managing the underlying aetiology as well as the wound bed. The International Leg Ulcer Advisory Board's recommended treatment pathway provides clear guidance on treatment choices and referral pathways according to the ulcer aetiology [35].
Measures to manage any co-existing medical conditions that may delay healing are integral to an effective framework of care. Margolis et al examined co-existing medical conditions in patients with venous disease and found asthma, congestive heart failure, diabetes, deep vein thrombosis, lower limb cellulitis, lower limb oedema, osteoarthritis, rheumatoid arthritis and peripheral vascular disease [36].
Although malnutrition is frequently linked to delayed healing [37] clinicians tend to be poor at assessing a patient's nutritional status [38] [39]. A balanced diet that includes protein, carbohydrates, fats, vitamins and minerals is important in effective wound bed preparation [40], while obesity is linked to increased risk of venous hypertension, arteriosclerosis, atherosclerosis and diabetes. The MUST tool (Malnutrition Universal Screening Tool) and the NICE nutrition guidelines provide useful frameworks for assessment and should be used to guide practice [38] [39].
Nurses are responsible for continually evaluating and recording the care they give [28] and for altering the treatment where appropriate. An effective framework of care should include clear treatment aims, including well-defined entry and exit points in order to avoid long-term use of ineffective therapies. Appropriate measures should be chosen to evaluate care, such as reduction in wound size, ability to tolerate compression or a reduction in limb circumference. Time frames for evaluation should be clearly identified and rationalised.
Important advances in leg ulcer management have been made in the past two decades in relation to leg ulceration, including provision of national and international guidelines [26] [31] [34] [41] [42] [43] [44], education, the availability of compression bandaging on UK prescription and an emerging understanding of wound bed preparation. Wound bed preparation and the TIME framework offer an important and systematic tool to aid chronic wound management. This must be used alongside an holistic approach, as stressed by Falanga [3]. Future work needs to focus on evaluating the effectiveness of such frameworks.
1. Harris IR, Yee KC, Walters CE, Cunliffe WJ, Kearney JN, Wood EJ, et al. Cytokine and protease levels in healing and non-healing chronic venous leg ulcers. Exp Dermatol 1995; 4(6): 342-9.
2. Greener B, Hughes AA, Bannister NP, Douglass J. Proteases and pH in chronic wounds. J Wound Care 2005; 14(2): 59-61.
3. Falanga V. Wound bed preparation: science applied to practice. In: European Wound Management Association (EWMA). Position Document. Wound Bed Preparation in Practice. London: MEP Ltd, 2004; available from URL: http://www.ewma.org/.
4. Vowden P, Vowden K, Investigations in the management of lower limb ulceration. In: White RJ, editor. Trends in Wound Care (British Journal of Nursing (BJN) Monograph). London: Quay Books, 2002.
5. Callam MJ, Ruckley CV, Harper DR, Dale JJ. Chronic ulceration of the leg: extent of the problem and provision of care. Br Med J (Clin Res Ed) 1985; 290(6485): 1855-6.
6. Cornwall JV, Dore CJ, Lewis JD. Leg ulcers: epidemiology and aetiology. Br J Surg 1986; 73(9): 693-6.
7. Nelzen O, Berbqvist D, Lindhagen A, Hallbrook T. Chronic leg ulcers: an underestimated problem in primary health care among elderly patients. J Epidemiol Community Health 1991; 45(3): 184-7.
8. Buxton PK. Leg ulcers. Br Med J 1987; 295(6612): 1542-5.
9. Franks PJ, Oldroyd MI, Dickson D, Sharp EJ, Moffatt CJ. Risk factors for leg ulcer recurrence: a randomized trial of two types of compression stocking. Age Ageing 1995; 24(6): 490-4.
10. Freak L, Simon D, Kinsella A, McCollum C, Walsh J, Lane C. Leg ulcer care: an audit of cost-effectiveness. Health Trends 1995-1996; 27(4): 133-6.
11. Persoon A, Heinen MM, van der Vleuten CJ, de Rooij MJ, van de Kerkhof PC, van Achterberg T. Leg ulcers: a review of their daily impact on life. J Clin Nurs 2004; 13(3): 341-54.
12. Lindsay E. The Lindsay Leg Club Model: a model for evidence-based leg ulcer management. Br J Community Nurs: 2004; June (Suppl): S15-20.
13. Ballard Wilson A. Quality of life and leg ulceration from the patient's perspective. In: Cutting KF, editor. Trends in Wound Care Volume IV. London: Quay Books, 2005.
14. Moffatt CJ, Franks PJ, Oldroyd M, Bosanquet N, Brown P, Greenhalgh RM, et al. Community clinics for leg ulcers and impact on healing. Br Med J 1992; 305(6866): 1389-92.
15. Ghauri AS, Nyamekye I, Grabs AJ, Farndon JR, Poskitt KR. The diagnosis and management of mixed arterial/venous leg ulcers in community-based clinics. Eur J Vasc Endovasc Surg 1998; 16(4): 350-5.
16. Moffatt CJ. Wound bed preparation in practice (editorial). In: European Wound Management Association (EWMA). Position Document. Wound Bed Preparation in Practice. London: MEP Ltd, 2004; available from URL: http://www.ewma.org/.
17. Dowsett C. The Wound Bed Preparation Cycle (presented at pre-conference symposia). Harrogate, UK: Wounds UK, 2004.
18. Morison M, Moffatt C. Leg ulcers. In: Morison M, Moffatt C, Bridel-Nixon J, Bale S, editors. A Colour Guide to the Nursing Management of Chronic Wounds. Second edition. London: Mosby, 1999.
19. Enoch S, Price P. Should alternative endpoints be considered to evaluate outcomes in chronic recalcitrant wounds? World Wide Wounds 2004; available from URL: http://www.worldwidewounds.com/2004/october/Enoch-Part2/Alternative-Enpoints-To-Healing.html.
20. Edwards LM. Why patients do not comply with compression bandaging. Br J Nurs 2003; 12(11 Suppl): S5-6, S8, S10.
21. Marston W, Vowden K. Compression therapy: a guide to safe practice. In: European Wound Management Association (EWMA). Position Document. Understanding Compression Therapy. London: MEP Ltd, 2003; available from URL: http://www.ewma.org/.
22. Dale JJ, Gibson B. Information will enhance compliance. Informing clients about compression hosiery. Prof Nurse 1992; 7(11): 755-6, 758-60.
23. Bale S, Harding K. Managing patients unable to tolerate therapeutic compression. Br J Nurs 2003; 12(19 Suppl): S4-13.
24. Bale S, Harding K, Managing patients unable to tolerate compression. In: White RJ, editor. Trends in Wound Care Volume III. London: Quay Books, 2004.
25. Moffatt C. Issues in the assessment of leg ulceration. J Wound Care 1998; 7(9): 469-73.
26. European Wound Management Association (EWMA). Position Document. Pain at Wound Dressing Changes. London: MEP Ltd, 2002; available from URL: http://www.ewma.org/.
27. World Union of Wound Healing Societies (WUWHS). Principles of Best Practice: Minimising Pain at Wound Dressing-related Procedures. A consensus document. London: MEP Ltd, 2004; available from URL: http://www.wuwhs.org/.
28. Nursing and Midwifery Council. The NMC Code of Professional Conduct: Standards for Conduct, Performance and Ethics. London: NMC, 2004.
29. Hollinworth H. Pain at wound dressing-related procedures: a template for assessment. World Wide Wounds 2005; available from URL: http://www.worldwidewounds.com/2005/august/Hollinworth/Framework-Assessing-Pain-Wound-Dressing-Related.html.
30. Callam MJ, Harper DR, Dale JJ, Ruckley CV. Chronic leg ulceration: socio-economic aspects. Scott Med J 1988; 33(6): 358-60.
31. Scottish Intercollegiate Guidelines Network. The Care of Patients with Chronic Leg Ulcer. National Clinical Guildline 26. Edinburgh: SIGN, 1998.
32. Ruckley CV, Dale JJ, Callam MJ, Harper DR. Causes of chronic leg ulcer. Lancet 1982; 2(8298): 615-616.
33. Tillman D, Uncommon causes of leg ulceration and lesions not to be missed. In: Cutting K, editor. Trends in Wound Care. Volume IV. London: Quay Books, 2006.
34. Royal College of Nursing. Clinical Practice Guidelines. The Nursing Management of Patients with Venous Leg Ulcers. Second edition. London: RCN, 2006.
35. European Wound Management Association (EWMA). Position Document. Understanding Compression Therapy. London: MEP Ltd, 2003; available from URL: http://www.ewma.org/.
36. Margolis DJ, Knauss J, Bilker W. Medical conditions associated with venous leg ulcers. Br J Dermatol 2004; 150(2): 267-73.
37. Russell L. The importance of patients' nutritional status in wound healing. In: White JR, editor. Trends in Wound Care. Volume II. London: Quay Books, 2003.
38. British Association for Parenteral and Enteral Nutrition. MUST (Malnutrition Universal Screening Tool) Nutritional Assessment Tool. Redditch: BAPEN, 2003; available from URL: http://www.bapen.org.uk/.
39. National Institute for Health and Clinical Excellence. Nutrition Support in Adults. NICE Guideline. London: NICE, 2006; available from URL: http://guidance.nice.org.uk/CG32.
40. Pinchcofsky-Devin G. Nutrition and wound healing. J Wound Care 1994; 3(5): 231-4.
41. Clinical Resource Efficiency Support Team. Guidelines for the Assessment and Management of Leg Ulceration. Belfast: Crest, 1998.
42. European Wound Management Association (EWMA). Position Document. Wound Bed Preparation in Practice. London: MEP Ltd, 2004; available from URL: http://www.ewma.org/.
43. European Wound Management Association (EWMA). Position Document. Identifying Criteria for Wound Infection. London: MEP Ltd, 2005; available from URL: http://www.ewma.org/.
44. European Wound Management Association (EWMA). Position Document. Management of Wound Infection. London: MEP Ltd, 2006; available from URL: http://www.ewma.org/.