
| R Chaffey Staff Nurse, Ward 1 Dermatology University Hospital of Wales Submitted: 6th October 1997 |
Contents History Initial treatment Introduction to larval therapy Conclusion Reference |
 Mrs Williams whose photograph is
reproduced with her permission.
Mrs Williams whose photograph is
reproduced with her permission.
Whilst on a Mediterranean holiday, she received an insect bite on her left foot which rapidly became infected causing her leg to become red and painful with swelling that extended to the knee.
The following day she was admitted to the local hospital where intravenous antibiotic therapy was initiated. Her condition continued to deteriorate, and after a few days the cellulitis had extended to her groin and the area below her knee had become covered with blisters.
Extensive sugical debridement of the the lower leg was performed without the benefit of anaesthetic or any form of analgesia - a procedure that caused Mrs Williams severe distress. The wounds were then cleaned with water and a silvadene dressing applied which was renewed daily.
Ten days later she was flown home to the United Kingdom.
Following this initial assessment, both wounds were treated with a hydrogel (Intrasite gel - Smith & Nephew Medical Ltd), and covered with a secondary dressing.
The following day she was seen by a consultant dermatologist who diagnosed cellulitis and lymphangitis (inflammation of the lymph vessels). Intravenous antibiotic therapy was commenced with benzylpenicillin and flucloxicillin. The wound on the outer aspect of the leg, which measured 22 x 9 cm, was dressed with an alginate dressing and the wound on the inner aspect, which measured 17 x 9 cm, was dressed with a hydrogel containing metronidazole.
Six days later both wounds had shown a slight improvement but the skin between remained erythematous although the blisters on her thigh had largely resolved. Treatment was continued as before and Mrs Williams was transferred to the dermatology ward.
Nine days after admission, Mrs Williams was given oral antibiotic therapy but this was poorly tolerated and discontinued after four days, so intravenous antibiotics were given once again. At this stage a biopsy of the wound was taken to exclude the possibility of pyoderma gangrenosum.
 Figure 1 - Mrs Williams hiding as
larvae were applied.
Figure 1 - Mrs Williams hiding as
larvae were applied.
Initially, because of Mrs William's reservations, only the wound on the medial aspect of her leg was treated with larvae. Prior to commencement of the treatment this wound was covered with a thick layer of sloughy (Figure 2).
 Figure 2 - Wound prior to
the application of larvae (31/10/96)
Figure 2 - Wound prior to
the application of larvae (31/10/96)
The larvae were applied using a dressing retention system described previously. [1]
The skin surrounding the wound was first protected by strips of a hydrocolloid sheet (Granuflex) approximately 2 cm wide. About 150 sterile larvae were gently rinsed out of the container in which they were supplied and placed on a piece of sterile net. This had been trimmed to overlap the edges of the wound by about 1 cm.
The net was then attached to the hydrocolloid dressing with adhesive tape ensuring the edge was completely sealed to prevent the maggots escaping.
The purpose of the hydrocolloid frame is to provide a skin-friendly base for the net, and protect the skin around the wound from the action of proteolytic enzymes produced by the larvae. It also stops the larvae from migrating on to intact skin, where they might cause a tickling sensation. Gauze swabs were moistened with sodium chloride solution 0.9% and placed on the outside of the net to ensure that the maggots did not dry out. The dressing was then covered with dressing pads secured into place with a bandage.
The dressing was left in place for 48 hours after which time the larvae were removed and the wound reassessed. Although some of the maggots had died, the amount of slough on the wound had been noticeably reduced.
The remaining maggots were washed off the wound with sodium chloride solution 0.9% and a second batch of larvae applied. On this occasion, the larvae were also introduced into to the second wound. As before these were left in place for 48 hours.
Upon removal of the outer dressing a marked reduction in the amount of slough present was noted (Figure 3).
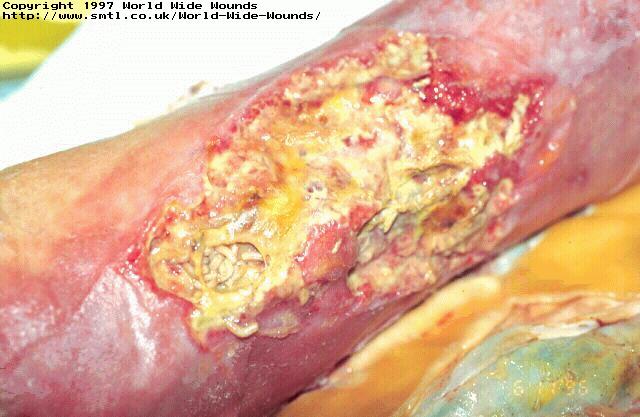 Figure 3 - Wound after 2
applications of larvae (6/11/96)
Figure 3 - Wound after 2
applications of larvae (6/11/96)
A further batch of larvae were then applied. At this stage Mrs Williams' intravenous antibiotic therapy was discontinued, and she was given oral therapy in the form of an elixir which she tolerated well.
The larvae were left in place for a further 48 hours. Once again, a significant number of larvae had died on both wounds, but those that survived had further reduced the amount of slough and necrotic tissue present.
Twenty days after admission, following a third cycle of larval therapy, the wounds showed considerable improvement (Figure 4).
 Figure 4 - Wound after 3
applications of larvae (8/11/96)
Figure 4 - Wound after 3
applications of larvae (8/11/96)
By this time, Mrs Williams had also overcome much of her initial dislike of the creatures. Unfortunately, however, she developed a further episode of cellulitis which necessitated a five day course of intravenous antibiotic therapy.
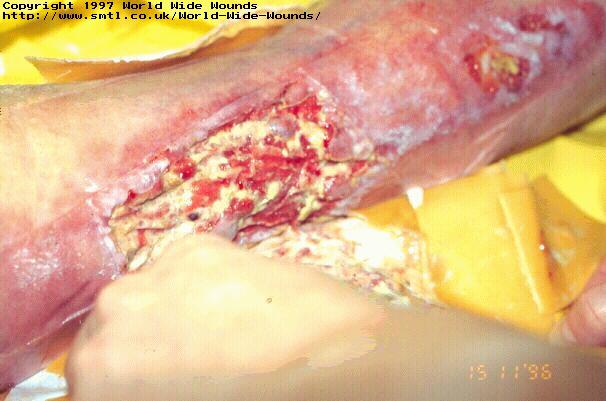 Figure 5 - Wound after 5
applications of larvae (15/11/96)
Figure 5 - Wound after 5
applications of larvae (15/11/96)
After a further four applications of larval therapy, on Mrs Williams' 30th day in hospital, the larval therapy was finally discontinued. At this stage the wounds were completely free of slough, with evidence of much new granulation tissue present. Conventional dressings were then applied to continue the healing process. Three days later antibiotic therapy was discontinued as the leg was pain free with no erythema present in the surrounding skin.
Conventional treatment was continued until Mrs Williams was discharged, although this was delayed for a week because of a flare up of her rheumatoid arthritis. Six weeks after discharge her wounds were virtually closed.
 Figure 6 - Wound during follow
up treatment photographed on 3/12/96
Figure 6 - Wound during follow
up treatment photographed on 3/12/96
The larvae made a major contribution to the successful treatment of this patient, removing the slough that formed a barrier to healing and a potential source of infective organisms. In this particular instance, however, debridement was slower than anticipated because of the unexplained high mortality rate of the maggots during the early stages of treatment.