Recent advances in the use of lasers in dermatology.
Lasers have been used in dermatology for more than 20 years. The
first lasers used were the Ruby and Argon lasers, and a great deal
of experience has been obtained particularly with the latter. The
Argon laser has been used predominantly in the treatment of
cutaneous vascular lesions and the CO2 laser both as a
cutting and ablating tool.
There have been significant advances in the development and use
of dermatological lasers. Much of this development stems from the
close co-operation of scientists and clinicians and laser
manufacturers. Today's lasers are more specifically designed for a
narrow range of applications and have significant advantages over
older lasers. This article will review the use of the
flashlamp-pulsed tunable dye laser in the treatment of port wine
stains, and developments in the treatment of tattoos and cutaneous
pigmented disorders, and skin resurfacing.
Flashlamp-pumped pulsed tunable dye
laser treatment.
For over 20 years, the Argon laser has been the most widely used
laser for the treatment of cutaneous vascular lesions [1]. The Argon laser emits blue and green light at
488 and 514 nm. These wavelengths of light are preferentially
absorbed by oxyhaemoglobin and melanin in the skin[2]. The light energy absorbed by erythrocytes
within blood vessels is converted to heat, leading to red cell
destruction and thrombosis of small blood vessels.
Port wine stains
Port wine stains [PWS] are benign vascular birthmarks which consist
of ectatic capillaries within the superficial dermis[3]. PWS persist throughout life and cause significant
psychological disability[4]. Light from the
Argon laser produces selective damage to the ectatic blood vessels
within a PWS and results in significant lightening of the skin[3,5]. Most large series of patients treated with
this laser have reported good and excellent results in 60 - 80% of
patients[6]. Best results have been in
dark purple PWS in adults, worst results in children with pink,
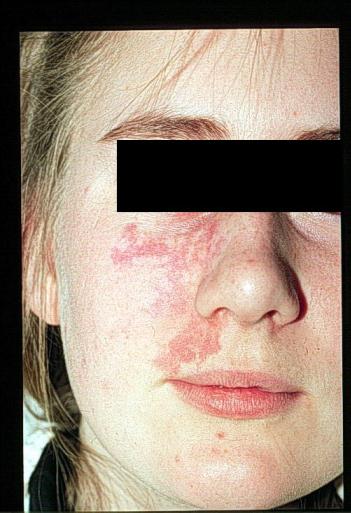
easily compressible PWS. Unfortunately the incidence of scarring
after Argon laser treatment is significant, with textural changes
occurring in up to 22% of patients. [Fig.1]
Fig. 1
Scarring after Argon laser treatment of a port wine stain 
(click on image for full size illustration)
Histological assessments of Argon laser treated PWS have
demonstrated that although the light is selectively absorbed by
haemoglobin, the damage induced is relatively non-specific[7,8]. These changes are in part due to
non-selective absorption of the Argon laser light by other
chromophores such as melanin, and diffusion of thermal energy away
from targeted blood vessels to adjacent structures due to the long
[ms] laser pulses employed[9]. Analysis of the
optical properties of PWS skin has suggested different parameters
to those of the Argon laser for successful treatment of these
naevi[10,11]. Light with a wavelength of 577
nm coincides with the beta absorption peak of oxyhaemoglobin and
was the original wavelength used in flashlamp-pumped pulsed dye
lasers[12]. Preliminary studies revealed
high response rates with minimal complications. Penetration depth
can be increased from 0.5 to 1.2 mm in PWS skin, whilst maintaining
the same degree of vascular selectivity, by increasing the
wavelength of light from 577 to 585 nm[13] .
It is possible to confine thermal injury to targeted blood vessels,
without heat diffusion to surrounding tissues, by using microsecond
pulses [Table 1].
Table 1: Treatment parameters of flashlamp-pumped pulsed dye
laser.
| Wavelength |
585nm |
| Pulse Duration |
450µs |
| Spot size |
5-10 mm |
| Energy fluence |
5-9 J/cm2 |
Histological studies have confirmed the selective vascular injury
induced by this laser with minimal damage to the overlying
epidermis. Videomicroscopic analysis of treated skin has confirmed
that there is no thermal damage to the epidermis[14].
The significant advantage of this laser is its safety and
efficacy in children with PWS and low incidence of scarring[15-17]. Treatment in older children and adults is
well tolerated, local anaesthesia (EMLA cream) often being
adequate[18]. Younger children may
require repeated general anaesthetics. The laser produces marked
bruising which can persist for up to 2 weeks, although crusting and
weeping is much less common than with other lasers.
Treatments to the whole port wine stain are generally repeated
every 6 - 12 weeks and a course of treatment is prolonged, 10 or
more treatments often being necessary. Not all patients will clear;
the site of the PWS will influence outcome[19]. Recent work analysing the pattern of vascular
ectasia within a PWS using a videomicroscope has identified
patterns of ectasia associated with good and poor outcomes from
pulsed dye laser therapy[20]. Patients with
ectasia of the superficial capillary loops had a better outcome
than those with ectasia of the horizontal vascular plexus. Further
work may enable a more accurate prognosis for outcome of treatment.
Best results have been on facial PWS and worst results on the lower
limbs[21]. [Fig 2a & b].
Fig. 2a & b. Facial port wine stain before and after pulsed
dye laser therapy
 click on image for full size
illustration
click on image for full size
illustration
Hyperpigmentation may be a problem, particularly following
treatment of PWS on the leg. Scarring is rare without additional
trauma in the post-treatment period[22].
This laser is also reported to be of value in hastening the
resolution of strawberry haemangiomas[23,24], particularly if the strawberry
haemangioma is causing complications such as ulceration or
bleeding, but controlled studies are lacking. Treatment should be
performed early for any benefit[25].
However the flashlamp-pumped dye laser can also produce
satisfactory changes in residual haemangiomas with a prominent
telangiectatic component.
Tattoos often applied in teenage years may become a source of
regret and a social burden in later life[26]. A number of methods of removal of tattoos have
been employed including dermabrasion, salabrasion, cryotherapy and
excision. Surgical excision of large tattoos requires skin
grafting. The other methods suffer from the disadvantages of
incomplete pigment removal, necessity of repeated procedures, pain
and frequent scarring. Carbon dioxide laser therapy[27] removes tattoo pigment after vaporization of
the epidermis and superficial dermis. Although effective, this
laser has a high incidence of scarring and pigmentary disturbances.
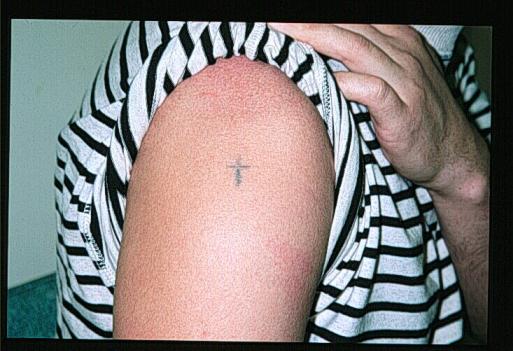
"Q-switching" whereby high energy levels [5 - 10 J/cm2]
delivered in ultrashort pulse widths [10 - 80 ns] of Ruby, Nd:YAG
and Alexandrite lasers has offered significant advances in the
treatment of tattoos, particularly blue-black amateur tattoos[28-30] [Fig 3a & b].
Fig. 3a & b. Amateur tattoo on shoulder treated once with the
Q-Switched Nd:YAG laser.
 click on image for full size
illustration
click on image for full size
illustration
The light emitted by these lasers interacts with dermal pigment
within tattoos and produce selective removal of the pigment, partly
by photomechanical disruption of the pigment granules[31]. Ruby lasers emit light at 694 nm and Nd:YAG
lasers at 1064 nm. Both lasers produce best results in blue-black
tattoo pigments. The Ruby laser can also be used to treat green
tattoos[32]. Frequency doubling of Nd:YAG
laser light halves the wavelength to 532 nm producing green light.
This green light can produce fading of red tattoo pigments[33]. The Alexandrite laser with a wavelength of
755 nm produces slower results than the other two Q-Switched lasers
but may be of value in the treatment of other coloured tattoo
pigments[34]. These lasers produce
much less epidermal reaction than other methods of tattoo removal
particularly if large laser beam diameters are used. There is a
consequent reduction in the incidence of scarring following
treatment. Hypopigmentation following Ruby laser treatment may be a
problem.
As melanin absorbs across a wide part of the electromagnetic
spectrum, older lasers with long pulse durations have been employed
with some success in the treatment of pigmented cutaneous lesions[35]. Non-specific thermal damage following
heat diffusion to other cutaneous structures resulted in scarring
in some cases. Q-Switched lasers have been used to treat cutaneous
pigmented lesions with some success[36-39]. Both
epidermal and dermal pigmented lesions may respond, such as cafe au
lait macules, lentigines and naevus of Ota [Fig 4a & b].
Fig. 4a & b. Benign lentigo treated twice with the Nd:YAG
laser.
 Click on image for full size
illustration
Click on image for full size
illustration 
Repeated treatments may be necessary and the lesion may recur.
There is insufficent data concerning laser treatment of benign
melanocytic naevi to recommend this form of treatment[40,41]. It is not possible currently to
determine which laser is more successful in this field as few
authors have presented data on large series of patients. However,
preliminary work from Japan on 200 naevus of Ota patients treated
with the Nd:YAG laser has revealed impressive results in some
patients[39]. Q-Switched lasers have a low
incidence of adverse reactions in this group of conditions. The
Alexandrite laser theoretically may also be of value in the
treatment of pigmented lesions although there is little published
clinical work to support this as yet. A flashlamp-pumped pulsed dye
laser emitting light at 510 nm has also been used in the treatment
of pigmented lesions[42,43]. Again
short pulse durations [300 ns] and high peak powers [approximately
4 MW] are utilised to produce selective photothermolysis of
pigment-containing cells.
Carbon Dioxide Laser
The carbon dioxide laser emits infrared light at 10,600 nm. This
wavelength is absorbed by tissue water and the laser produces
non-selective thermal damage of tissue. This laser is used widely
in gynaecological surgery and has been used to treat a number of
dermatological disorders. The laser can be used in focused mode
with a small spot size and high energy densities to cut tissue
haemostatically as small blood vessels are sealed thermally. In the
defocused mode, with a spot size of 2 mm, the laser can be used for
superficial vapourisation under local anaesthesia[44]. A variety of skin diseases have been treated
with this laser[45-48]. This laser has a
relatively high incidence of scarring and other hazards include
human papilloma virus DNA present in the smoke plume generated when
treating warts[49] [Fig 5].
Fig. 5 Smoke plume during CO2 treatment of verruccae
 click on image for full size
illustration
click on image for full size
illustration
A resurgence of interest has developed in the CO2 laser
by the use of ultrapulses of the light. Pulse durations of 250
µs are delivered which allows thermal destruction of the
epidermis and superficial dermis without thermal diffusion to
deeper tissue. The laser can be linked to an optomechanical scanner
for improved results. The laser has an increasing role in the
treatment of photodamaged skin and rhytides[50]. Both ablation of tissue and dermal shrinkage
are considered important mechanisms in the improvement of
photodamaged skin[51]. The latter has
been measured objectively[52]. Careful pre
and post operative preparations are necessary to reduce the risk of
adverse reactions which include scarring, post inflammatory
pigmentary disturbances, persisting erythema, bacterial and viral
infections.
The newer generation of lasers with short pulse durations and high
peak powers are capable of more selective destruction of target
chromophores. More appropriate wavelength selection for different
cutaneous disorders has resulted in a modest improvement in results
of treatment and a substantial reduction in adverse reactions such
as scarring and pigmentary disturbances. The flashlamp-pulsed dye
laser has enabled the safe treatment of young children with PWS,
and Q-Switched lasers have been effective in the treatment of a
number of cutaneous pigmented disorders, in particular blue-black
tattoos. Further research will clarify which, if any, is the "best"
laser in this second group; significant advances in technology and
clinical results offer an optimistic future in this field.
The author acknowledges the support of the Disfigurement Guidance
Centre, Cupar, Fife, Scotland.
- Spicer M S, Goldberg D J. Lasers in
dermatology. J Am Acad Dermatol 1996; 34: 1 - 25. PubMed
Abstract:
http://www.ncbi.nlm.nih.gov/htbin-post/Entrez/query?uid=8543678&form=6&db=m&Dopt=r
- Anderson, R. R., Parrish, J. A. The
optics of human skin. J Invest Dermatol 1981; 77: 13 - 19.
PubMed Abstract:
http://www.ncbi.nlm.nih.gov/htbin-post/Entrez/query?uid=7252245&form=6&db=m&Dopt=r
- Noe, J. M., Barsky, S. H., Geer, D. E.,
Rosen, S. Port wine stains and the response to argon laser therapy:
successful treatment and the predictive role of colour, age and
biopsy. Plast Reconstr Surg 1980; 65: 130 - 36. PubMed
Abstract:
http://www.ncbi.nlm.nih.gov/htbin-post/Entrez/query?uid=7352152&form=6&db=m&Dopt=r
- Lanigan, S. W., Cotterill, J. A.
Psychological disabilities amongst patients with port wine stains.
Br J Dermatol 1989; 121: 209 - 215. PubMed Abstract:
http://www.ncbi.nlm.nih.gov/htbin-post/Entrez/query?uid=2775645&form=6&db=m&Dopt=r
- Carruth, J. A. The argon laser in the
treatment of vascular naevi. Br J Dermatol 1982; 107: 365 -
368.
- Apfelberg, D. B., Flores, J. T.,
Maser, M. R., Lash, H. Analysis of complications of argon laser
treatment of port wine haemangiomas with reference to striped
technique. Lasers Surg Med 1983; 2(4): 357 - 371. PubMed
Abstract:
http://www.ncbi.nlm.nih.gov/htbin-post/Entrez/query?uid=6865639&form=6&db=m&Dopt=r
- Finley, J. L., Arndt, K. A., Noe, J.,
Rosen, S. Argon laser - port wine stain interaction. Immediate
effects. Arch Dermatol 1984; 120: 613 - 619. PubMed
Abstract:
http://www.ncbi.nlm.nih.gov/htbin-post/Entrez/query?uid=6372699&form=6&db=m&Dopt=r
- Greenwald, J., Rosen, S., Anderson, R.
R. et al. Comparative histological studies of the tunable dye [at
577 nm] laser and argon laser. The specific vascular effects of the
dye laser. J Invest Dermatol 1981; 77(3): 305 - 310. PubMed
Abstract:
http://www.ncbi.nlm.nih.gov/htbin-post/Entrez/query?uid=7264364&form=6&db=m&Dopt=r
- Tan, O. T., Carney, M., Margolis, R., et al.
Histologic responses of port-wine stains treated by argon, carbon
dioxide and tunable dye lasers. Arch Dermatol 1986; 122(9):
1016 - 1022. PubMed Abstract:
http://www.ncbi.nlm.nih.gov/htbin-post/Entrez/query?uid=3090945&form=6&db=m&Dopt=r
- Van Gemert, M. J. C., Welch, A. J.
Treatment of port-wine stains: analysis. Med Instrum 1987;
21(4): 213 - 217. PubMed Abstract:
http://www.ncbi.nlm.nih.gov/htbin-post/Entrez/query?uid=3452741&form=6&db=m&Dopt=r
- Anderson, R. R., Parrish, J. A.
Microvasculature can be selectively damaged using dye lasers: a
basic theory and experimental evidence in human skin. Lasers
Surg Med 1981; 1(3): 263 - 76. PubMed Abstract:
http://www.ncbi.nlm.nih.gov/htbin-post/Entrez/query?uid=7341895&form=6&db=m&Dopt=r
- Morelli, J. G., Tan, O. T., Garden, J
et al. Tunable dye laser [577 nm] treatment of port wine stains.
Lasers Surg Med 1986; 6: 94 - 99. PubMed Abstract:
http://www.ncbi.nlm.nih.gov/htbin-post/Entrez/query?uid=3959722&form=6&db=m&Dopt=r
- Tan, O. T., Murray, S., Kurban, A. K.
Action spectrum of vascular specific injury using pulsed
irradiation. J Invest Dermatol 1989; 92: 868 - 71. PubMed
Abstract:
http://www.ncbi.nlm.nih.gov/htbin-post/Entrez/query?uid=2723451&form=6&db=m&Dopt=r
- Motley, R. J., Katugampola, G, Lanigan,
S. W. Microvascular abnormalities in port wine stains and response
to 585 nm pulsed dye laser treatment. Br J Dermatol 1996;
135: Suppl 47: 13 - 14.
- Garden, J. M., Polla, L. L., Tan, O. T.
The treatment of port-wine stains by the pulsed dye laser. Arch
Dermatol 1988; 124: 889 - 96. PubMed Abstract:
http://www.ncbi.nlm.nih.gov/htbin-post/Entrez/query?uid=3377518&form=6&db=m&Dopt=r
- Polla, L. L., Tan, O. T., Garden, J. M.,
Parrish, J. A. Tunable pulsed dye laser for the treatment of benign
cutaneous vascular ectasia. Dermatologica 1987; 174: 11 -
17. PubMed Abstract:
http://www.ncbi.nlm.nih.gov/htbin-post/Entrez/query?uid=2433166&form=6&db=m&Dopt=r
- Tan, O. T., Sherwood, K., Gilchrest, B. A.
Treatment of children with port wine stains using the
flashlamp-pulsed tunable dye laser. N Engl J Med 1989; 320:
416 - 21. PubMed Abstract:
http://www.ncbi.nlm.nih.gov/htbin-post/Entrez/query?uid=2913507&form=6&db=m&Dopt=r
- Lanigan, S. W., Cotterill, J. A. Use
of a lignocaine-prilocaine cream as an analgesic in dye laser
treatment of port wine stains. Lasers Med Science 1987; 2:
87 - 89.
- Renfro, L., Geronemus, R. G. Anatomical
differences of port-wine stains in response to treatment with the
pulsed dye laser. Arch Dermatol 1993; 129: 182 - 188. PubMed
Abstract:
http://www.ncbi.nlm.nih.gov/htbin-post/Entrez/query?uid=8434975&form=6&db=m&Dopt=r
- Motley, R. J., Katugampola, G., Lanigan,
S. W., Videomicroscopy of vascular patterns in port wine stains
predicts outcome. Lasers Surg Med 1996; Suppl 8: 94 -
99.
- Lanigan, S. W., Port wine stains on the
lower limb: response to pulsed dye laser therapy. Clin Exp
Dermatol 1996; 21: 88 - 92. PubMed Abstract:
http://www.ncbi.nlm.nih.gov/htbin-post/Entrez/query?uid=8759191&form=6&db=m&Dopt=r
- Swinehart, J.M., Hypertrophic
scarring resulting from flashlamp-pumped pulsed dye laser surgery.
J Am Acad Dermatol 1991; 25: 845 - 46.
- Glassberg, E., Lask, G., Rabinowitz,
L. G., Tunnessen, W. W. Capillary haemangiomas: case study of a
novel laser treatment and a review of therapeutic options. J
Dermatol Surg Oncol 1989; 15: 1214 - 1223. PubMed Abstract:
http://www.ncbi.nlm.nih.gov/htbin-post/Entrez/query?uid=2808890&form=6&db=m&Dopt=r
- Garden, J. M., Bakus, A. D., Paller, A.
S. Treatment of cutaneous haemangiomas by the flashlamp-pulsed dye
laser: Prospective analysis. J Pediatr 1992; 120: 555 - 60.
PubMed Abstract:
http://www.ncbi.nlm.nih.gov/htbin-post/Entrez/query?uid=1552392&form=6&db=m&Dopt=r
- Barlow, R. J., Walker, N. P. J., Markey,
A. C., Treatment of proliferative haemangiomas with the 585 nm
pulsed dye laser. Br J Dermatol 1996; 134: 700 - 704. PubMed
Abstract:
http://www.ncbi.nlm.nih.gov/htbin-post/Entrez/query?uid=8733375&form=6&db=m&Dopt=r
- Varma, S., Lanigan, S. W. The
psychological, social and financial burden of tattoos. Br J
Dermatol 1996; 135: Suppl 47: 37.
- Lanigan, S. W., Sheehan-Dare, R. A.,
Cotterill, J. A. The treatment of decorative tattoos with the
carbon dioxide laser. Br J Dermatol 1989; 120: 819 - 825.
PubMed Abstract:
http://www.ncbi.nlm.nih.gov/htbin-post/Entrez/query?uid=2757942&form=6&db=m&Dopt=r
- Reid, W. H., Miller, I. D., Murphy, M. J.,
Paul, J. P. and Evans, J. H. Q-Switched ruby laser treatment of
tattoos, a 9-year experience. Br J Plast Surg 1990; 43: 663
- 669. PubMed Abstract:
http://www.ncbi.nlm.nih.gov/htbin-post/Entrez/query?uid=2257415&form=6&db=m&Dopt=r
- Taylor, C. R., Gange, R. W., Dover, J.
S. et al. Treatment of tattoos by Q-Switched ruby laser. Arch
Dermatol 1990; 126: 893 - 899. PubMed Abstract:
http://www.ncbi.nlm.nih.gov/htbin-post/Entrez/query?uid=2360836&form=6&db=m&Dopt=r
- Kilmer, S. L., Anderson, R. R. Clinical
use of the Q-Switched ruby and the Q-Switched Nd:YAG [1064 nm and
532 nm] lasers for the treatment of tattoos. J Dermatol Surg
Oncol 1993; 19: 330 - 338. PubMed Abstract:
http://www.ncbi.nlm.nih.gov/htbin-post/Entrez/query?uid=8478472&form=6&db=m&Dopt=r
- Taylor, C. R., Anderson, R. R., Gange,
R. W. et al. Light and electron microscope analysis of tattoos
treated by Q-Switched ruby laser. J Invest Dermatol 1991;
97: 131 - 6. PubMed Abstract:
http://www.ncbi.nlm.nih.gov/htbin-post/Entrez/query?uid=2056183&form=6&db=m&Dopt=r
- Lowe, N. J. Laser therapy of vascular
benign pigmented lesions and tattoos. In: Marks, R., Cunliffe, W.
J. [eds], Skin Therapy. London: Martin Dunitz, 1994.
- Kilmer, S. L., Lee, M., Farinelli, W. et
al. Q-Switched Nd:YAG laser [1064 nm] effectively treats Q-Switched
ruby laser resistant tattoos. Lasers Surg Med 1992; Suppl.
4: 72.
- Fitzpatrick, R. E. Comparison of
the Q-Switched ruby, Nd:YAG and alexandrite lasers in tattoo
removal. Lasers Surg Med 1994; Suppl 6: 52.
- Apfelberg, D. B., Maser, M. R., Lash,
H., Rivers, J. The argon laser for cutaneous lesions. JAMA
1981; 245: 2073 - 5. PubMed Abstract:
http://www.ncbi.nlm.nih.gov/htbin-post/Entrez/query?uid=7230406&form=6&db=m&Dopt=r
- Taylor, C. R., Flotte, T. J., Gange, W.
R., Anderson, R. R. Treatment of naevus of Ota by Q-Switched ruby
laser. J Am Acad Dermatol 1994; 30: 743 - 751. PubMed
Abstract:
http://www.ncbi.nlm.nih.gov/htbin-post/Entrez/query?uid=8176014&form=6&db=m&Dopt=r
- Geronemus, R. G., Ashinoff, R. Use of
the Q-Switched ruby laser to treat tattoos and benign pigmented
lesions of the skin. Lasers Surg Med 1991; Suppl. 3, 64 -
5.
- Ashinoff, R., Levine, V., Tse, Y.,
McClain, S. Removal of pigmented lesions: comparison of the
Q-Switched ruby and neodynium: YAG lasers. Lasers Surg Med
1994; Suppl. 6: 50.
- Kasai, K-I., Notodihardjo, H. W. Analysis
of 200 nevus Ota patients who underwent Q-Switched Nd:YAG laser
treatment. Lasers Surg Med 1994; Suppl. 6: 50.
- Goldberg, D. J., Stampien, T.
Q-switched ruby laser treatment of congenital naevi. Arch
Dermatol 1995; 131: 621 - 623.
- Waldorf, H. A., Kauvar, A. N. B.,
Geronemus, R. G. Treatment of small and medium congenital naevi
with the Q-switched ruby laser. Arch Dermatol 1996; 132: 301
- 306. PubMed Abstract:
http://www.ncbi.nlm.nih.gov/htbin-post/Entrez/query?uid=8607635&form=6&db=m&Dopt=r
- Ruiz-Esparza, J., Fitzpatrick, R.
E., Goldman, M. P. Selective melanothermolysis: a histological
study of the Candela 510 nm pulsed dye laser for pigmented lesions.
Lasers Surg Med 1992; Suppl. 4: 73.
- Fitzpatrick, R. E., Goldman, M. P.,
Ruiz-Esparza, J. Treatment of benign cutaneous pigmented lesions
with the Candela 510 nm pulsed laser. Lasers Surg Med 1992;
Suppl. 4: 73.
- Reid, R. Physical and surgical principles
governing carbon dioxide laser surgery on the skin. Dermatol
Clin 1991; 9: 297 - 316.
- McBurney, E. I., Rosen, D. A. Carbon
dioxide laser treatment of verrucae vulgares. J Dermatol Surg
Oncol 1984; 10: 45 - 8. PubMed Abstract:
http://www.ncbi.nlm.nih.gov/htbin-post/Entrez/query?uid=6418779&form=6&db=m&Dopt=r
- Street, M. L., Roenigk, R. K.
Recalcitrant periungual verrucae; the role of carbon dioxide laser
vaporization. J Am Acad Dermatol 1990; 23: 115 - 20. PubMed
Abstract:
http://www.ncbi.nlm.nih.gov/htbin-post/Entrez/query?uid=2114426&form=6&db=m&Dopt=r
- Apfelberg, D. B., Maser, M. R., Lash,
H, et al. Treatment of xanthelasma palpebrarum with carbon dioxide
laser. J Dermatol Surg Oncol 1987; 13: 149 - 51. PubMed
Abstract:
http://www.ncbi.nlm.nih.gov/htbin-post/Entrez/query?uid=3805477&form=6&db=m&Dopt=r
- David, L. M. Laser vermilion ablation for
actinic cheilitis. J Dermatol Surg Oncol 1985; 11: 605 - 8.
PubMed Abstract:
http://www.ncbi.nlm.nih.gov/htbin-post/Entrez/query?uid=4008733&form=6&db=m&Dopt=r
- Garden, J. M., O'Banion, M. K.,
Shelnitz, L. S. et al. Papillomavirus in the vapor of carbon
dioxide laser-treated verrucae. JAMA 1988; 259: 1199 - 202.
PubMed Abstract:
http://www.ncbi.nlm.nih.gov/htbin-post/Entrez/query?uid=2828703&form=6&db=m&Dopt=r
- Hruza, G. J. and Dover, J. S. Laser skin
resurfacing. Arch Dermatol 1996; 32: 451 - 458.
- Wheeland, R. G. Clinical uses of
lasers in dermatology. Lasers Surg Med 1995; 16[1]: 2 - 23.
PubMed Abstract:
http://www.ncbi.nlm.nih.gov/htbin-post/Entrez/query?uid=7715398&form=6&db=m&Dopt=r
- Gardner, E. S., Reinisch, L.,
Stricklin, G. P. and Ellis, D. L. In vitro changes in non-facial
human skin following CO2 laser resurfacing. Lasers
Surg Med 1996; 19: 379 - 387. PubMed Abstract:
http://www.ncbi.nlm.nih.gov/htbin-post/Entrez/query?uid=8982996&form=6&db=m&Dopt=r
All materials
copyright © 1992-Feb 2001 by SMTL, March 2001 et seq by SMTL
unless otherwise stated.
|
Home |
Index |
Subject Areas |
SMTL |
Site Map |
Archive |
Contact Us
|
http://www.worldwidewounds.com/1997/july/Lanigan/Lanigan.html
Last Modified: Tuesday, 11-Dec-2001 11:40:38 GMT


 click on image for full size
illustration
click on image for full size
illustration
 click on image for full size
illustration
click on image for full size
illustration
 Click on image for full size
illustration
Click on image for full size
illustration 
 click on image for full size
illustration
click on image for full size
illustration